As a chaplain, and as a friend, I often tell others, “Loss is unavoidable—the best thing we can do is show up and accompany each other through it.” Today I invite you to accompany me through the loss of my dear friend Rosalie.
Rosalie has already been introduced to readers of Elder Chaplain, as she was a central character in my 2025 post “Here for Each Other.” I invite you to revisit this post now for additional insights into my remarkable friend. As mentioned there, the first impression Rosalie made on me was during a Quaker meeting in 2006, when she shared movingly of how she was coping with her metastatic breast cancer. What I didn’t mention is that, six months prior to that post, Rosalie’s cancer sprang back to life. It had spread throughout her bones, and this time there would be no respite. Rosalie died earlier this month, surrounded by family.
Of all the words I might choose to describe Rosalie, “caring” and “integrity” rise to the top. Rosalie was a physician, and caring is what she did in all dimensions of her life. Her outward demeanor was reserved, and she could be direct to the point of bluntness, but her heart for life and for healing shone through. Early in our relationship, she asked if she could speak with me privately as a larger meeting was breaking up. She said, “You’ll need paper and a pen.” She then proceeded, “You’re having your hip replaced next month. Here are the things you’ll need that your surgeon may not be thinking of.” Her recommendations, from icing machines to constipation remedies, proved invaluable.
Rosalie and I often served together on spiritual care committees for others at our Quaker meeting, and for several years we both participated in a group called Shepherds, focused on the broader needs of our community. Rosalie frequently identified needs that no one else had noticed, and took actions that made sure those people felt seen and supported. As mentioned in my earlier post, Rosalie convened a care committee for me when I was diagnosed with prostate cancer. And she accepted my offer to convene a care committee for her when her cancer returned.
When Rosalie’s oncologist came into their first appointment after imaging showed a return of her cancer, she handed Rosalie a treatment plan involving aggressive chemotherapy. Rosalie said she’d had Taxol before—and it was awful. Speaking doctor to doctor, she asked: What is midpoint of the bell curve of survival under the proposed plan? Around five years. And if she chose not to follow the treatment plan? Two and a half years. Rosalie felt she’d rather have two and a half good years than five years of potential misery. And that was that.
Rosalie’s perspective was one of profound gratitude. “Of course I’d rather live a longer life, but mostly I’m thankful for the 18 years I was given after my initial diagnosis and treatment. Then, my daughter was in high school; now, I’m going to see her get married. I’ve been given so much life over these 18 years, how could I complain I didn’t get more?” It’s a gift to be in the presence of someone as deeply grounded as Rosalie.
After a roller coaster of treatments intended (and sometimes succeeding) in improving her quality of life, Rosalie entered hospice last November. Soon she felt much less pain. A few weeks later she sent me an astonishing email, entitled “What Shall I Do While Waiting to Die?” Her goals:
- Increase my aqua jogging time slowly to 30 minutes (from 20 now)
- Step dance holding on to the refrigerator handles three times a day
- Finish another baby quilt
- Wait for spring to arrive so that I can again walk in the garden
- Smile a lot and try not to watch people’s amazement when I tell them that I am in hospice
I’m so happy she had the chance to accomplish all of these goals during her remaining months.
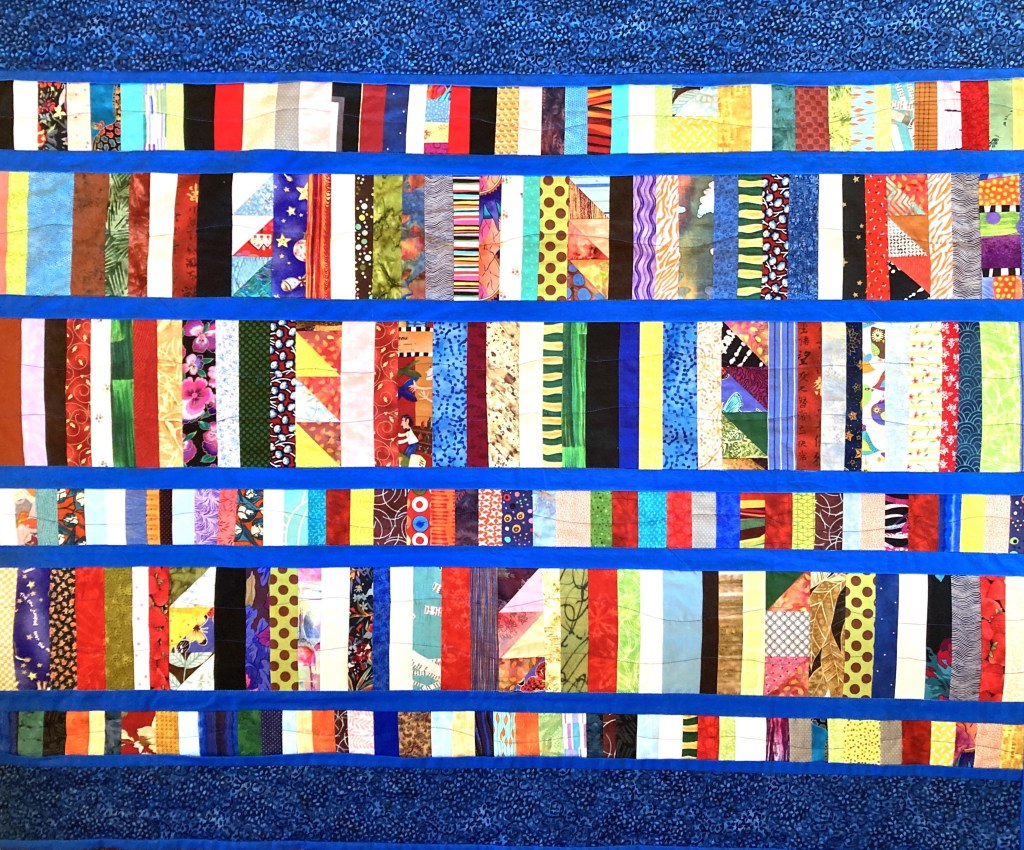
Which brings me to the topic of quilts … The photo accompanying this post is of the quilt Rosalie gave me when I was recovering from surgery for my prostate cancer. She made one for my daughter after she underwent a difficult surgery. She made a large one for our Quaker community to remember her by, and when she presented it to the community last September, she shared these words. “I love giving away things that I have made. It gives me joy to think that someone will warm their knees under a quilt that I have made.” (As I have, countless times.) She continued, “Many of my quilts have spoken to me over the years about community, and this one also speaks of community. That each of us has a unique gift to each other, and together—together—we make something greater, stronger, and more beautiful.” I have learned so much from Rosalie about how to be in community, and I have sought to emulate her spirit as I nurture my own communities.
Rosalie began that presentation by quoting from a card she had received, which she thought captured well how she tried to approach quilting. I think it applies equally well to how she approached life.
Advice From a Glacier
Carve your own path
Go slow
Channel your strengths
Smooth the way for others
Keep moving forward
Avoid meltdowns
Be cool